
More Information
Submitted: December 09, 2024 | Approved: December 18, 2024 | Published: December 19, 2024
How to cite this article: Sárközi L, Hegedűs A, Péterfi I. Newly Modified Posterior Axilla Maneuver: Tilt and Kristeller Procedure. Clin J Obstet Gynecol. 2024; 7(4): 125-129. Available from: https://dx.doi.org/10.29328/journal.cjog.1001179
DOI: 10.29328/journal.cjog.1001179
Copyright License: © 2024 Sárközi L, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Shoulder dystocia; Posterior axilla maneuver; Posterior axilla traction; Macrosomia

Newly Modified Posterior Axilla Maneuver: Tilt and Kristeller Procedure
László Sárközi1*, András Hegedűs1 and István Péterfi2
1Department of Obstetrics and Gynaecology, Somogy County Kaposi Mór Teaching Hospital, Kaposvár, Hungary
2Head of Department, Department of Obstetrics and Gynaecology, Somogy County Kaposi Mór Teaching Hospital, Kaposvár, Hungary
*Address for Correspondence: László Sárközi, MD, Department of Obstetrics and Gynaecology, Somogy County Kaposi Mór Teaching Hospital, 7400 Kaposvár, Tallián Gy. u. 20-32, Kaposvár, Hungary, Email: [email protected]
Shoulder dystocia is a rare but severe complication of vaginal delivery with possibly serious consequences. Certain risk factors are associated with shoulder dystocia, but a general forecasting model is lacking. We present a Case report using a newly modified Posterior Axilla Maneuver technique that saved a 5.140 g (11 lbs. 5 oz.) newborn from shoulder dystocia. The child was born with Apgar 7/9, pH 7.17. Currently, there are no signs of any long-term sequelae.
Our procedure comprised the following steps: 1. First, we pulled the posterior shoulder downwards - in the direction and to the outer surface of the perineum. 2. Then we pulled the posterior shoulder backward - toward the maternal spine - when it was already outside the perineum and finished extracting the posterior shoulder. 3. By completing the first two steps, a Tilt of the shoulder girdle was reached in the midsagittal plane, resulting in a backward slope for the shoulder girdle so that the anterior shoulder touched the symphysis slightly from the back in a skewed manner, freeing it from the initial impacted position. 4. We applied the Kristeller procedure only after dislodging the anterior shoulder from its initial impacted position. 5. We also applied the McRoberts Maneuver at the end of the process to increase the diameter of the birth canal.
Shoulder dystocia
The definition and diagnosis of shoulder dystocia vary. We diagnosed shoulder dystocia after a visibly large head was delivered. We proceeded with the internal examination and found that the anterior shoulder was not accessible, i.e., stuck high above the symphysis, while the posterior shoulder was accessible. Hence, the shoulder girdle was in the anterior-posterior diameter. So, the diagnosis was based on the internal examination. This also meant that a usual stepwise approach was skipped to save time.
The treatment of shoulder dystocia also varies. There are external maneuvers, internal maneuvers, and salvage procedures. Many protocols exist, consisting of various orders of required events and maneuvers. The usual consensus is that the Kristeller procedure, i.e., fundal pressure, is not allowed in shoulder dystocia when the anterior shoulder is still impacted.
External maneuvers consist of the McRoberts maneuver, the Gaskin maneuver, the Rubin I. maneuver, a.k.a. supra symphyseal pressure, and the Walcher’s hanging position [1].
The internal maneuvers comprise the ancient Bourgois-Siegemund maneuver [2], the Couder’s maneuver [3] and the anterior axilla maneuvers, i.e., relieving the anterior shoulder and arm, a.k.a. Rubin II. maneuver; the relieving of the posterior shoulder and arm, a.k.a. Jacquemier's maneuver, the Posterior Axilla maneuvers [4], including the Willughby maneuver (17th century) [5] – a rotational maneuver, the Holman maneuver [6] – a forerunner of the tilt idea without the posterior axilla pull supplemented with the suprapubic pressure, the Schramm maneuver [7] – a rotation and traction, the Menticoglou maneuver [8] – the manual pull of the posterior axilla and delivery of the posterior arm, and the Hofmeyr and Cluver maneuver [9-13] – the posterior axillar pull with a catheter sling supplemented with the rotation by the sling and a push on the anterior shoulder with a finger when required; the Shoulder Shrug maneuver [14] – posterior shoulder shrug and rotation; the Zavanelli procedure and the Woods procedure.
The rescue maneuvers are the fracture of the clavicle, the symphysiotomy, and emergency laparotomy or cesarean section. The obsolete dissecting procedures of the infant are also salvage maneuvers.
We believe that shoulder dystocia is also a psychiatric event for the mother and her family, as well as the medical staff. This latter should also be emphasized in the future for better management outcomes.
Why an update of the Posterior Axilla Maneuvers could be useful?
Posterior Axilla Maneuvers are among the best procedures for shoulder dystocia management [15,16]. They offer the highest chance of resolving shoulder dystocia and cause fewer plexus and other injuries [17,18] compared to other maneuvers [3,19,20].
Published reports on successful management of shoulder dystocia in vaginal birth with above 5.000 g neonates are hard to find. One reason is that known macrosomia of that extent indicates a primary cesarean section [21]. Another reason could be that vaginal birth with shoulder dystocia above 5.000 g represents a nearly impossible mission [22] to complete successfully. This suggests that current shoulder dystocia maneuvers may have an upper limit of feasibility regarding infants’ birth weight.
Posterior Axilla Maneuvers are good. According to L. Ansell [15,23], Axillary traction procedures have a success rate of 95.8%, and Posterior arm delivery has a success rate of 85.7% and, in combination, even higher. Although these success rates are very high, sadly, each case that is not saved burdens all participants. It could be a reason why an update on Posterior Axilla Maneuvers may be needed for these cases.
Most shoulder dystocia cases are unpredictable. They can occur in a wide range of fetal birth weights, from below 4,000 g [18] to above 5,000 g. Real-time fetal weight estimates are imperfect, and birth could alter the size of the engaged head [17]. Despite all careful preparations, extremely macrosomia infants could still go into labor and have a higher risk of shoulder dystocia.
The existing maneuvers, including the known and practiced Posterior Axilla Maneuvers, do not apply to all shoulder dystocia deliveries, especially severe macrosomia cases—they were not designed or tested for them. In emergencies, however, they are the only tools available to upgrade to a desperate situation in real time. We believe a planned, careful update in Posterior Axilla Maneuvers could broaden the scope of the management tools.
The authors agree with M. Robson‘s statement [24]: “Most babies over 4.5 kg deliver without SD, and some cases of SD occur in babies < 4 kg. If we cannot predict and prevent SD, we need to be better prepared to manage it when it occurs.”
All Posterior Axilla Maneuvers imply an alternative birth mechanism regarding the driving force and the extent of movement of the joints involved. The birth mechanism originally described by Sellheim includes head movements involving the cervical and thoracal spines, resulting in the fetal head's descent, flexion, and rotation. Like all Posterior Axilla Maneuvers, our proposed mechanism focuses on movements of the thoracal spine, scapula, clavicle, sternum, and humerus. Our method exaggerates this function. Similar movements, however, could also occur in the birth process of preterm, low-birth-weight infants. Incorporating the above-mentioned movement characteristics into simulation models could also help design a new generation of mannequins serving teaching purposes [25].
Mrs. B.B. (born on 16.04.1993 herself from Shoulder Dystocia with clavicle fracture, G3/P1, previously gave birth to a 4.200 g newborn without complications in 2021) presented at 40 weeks + 1 day of pregnancy with labor pains at our hospital delivery room in 2024. On admission, the cervix was 4 cm in width, and the membranes were unruptured. Any accompanying illness to mention was a stable M.S. We used oxytocin infusion, and after the median-lateral episiotomy, the head was delivered. We noticed the large head and started to treat shoulder dystocia without delay. After exhausting the usual methods, we tried to modify existing posterior axilla maneuvers [4,6,8].
Upon entering the vagina with the first hand, we could reach the posterior shoulder and the posterior arm. Then, we could move our internal hand up along the posterior arm. With one hand in the vagina, we were not able to move the trunk, neither the posterior arm nor the posterior forearm. Changing hands and now the second hand in the vagina, only the front-facing side of the neck was available to palpate. We could not reach the anterior shoulder, nor was the anterior arm still single-handed. Let's now define the shoulder girdle line as horizontal.
After changing hands again, now with the first hand in the vagina, we could reach the posterior shoulder. We could grasp 90% under the posterior Armpit and pull the posterior shoulder downwards and outwards, delivering the posterior shoulder to the outer surface of the perineum.
After fully extracting the posterior shoulder and no hands in the vagina, we could enter the vagina with the second hand.
The first, posterior hand outside the vagina, pulled the posterior shoulder to the back of the mother, and the second, anterior hand inside the vagina, pushed the front-facing side of the neck at the shoulder beginning to the back of the mother. This coordinated effort of the two hands could move the stalled trunk to the back of the mother approximately—1 cm in length.
The posterior shoulder was pulled down, and the anterior shoulder was in its original position. The shoulder girdle line is now sloped backward relative to the initial 'horizontal' line (Figure 1). This change of direction in the impacted anterior shoulder line offered hope that Kristeller-type pushing from the fundus may cause the formerly perpendicularly impacted, now somewhat backward-tilted anterior shoulder line and surface to slide backward and downward against a slightly back-skewed-edged surface of the symphysis.
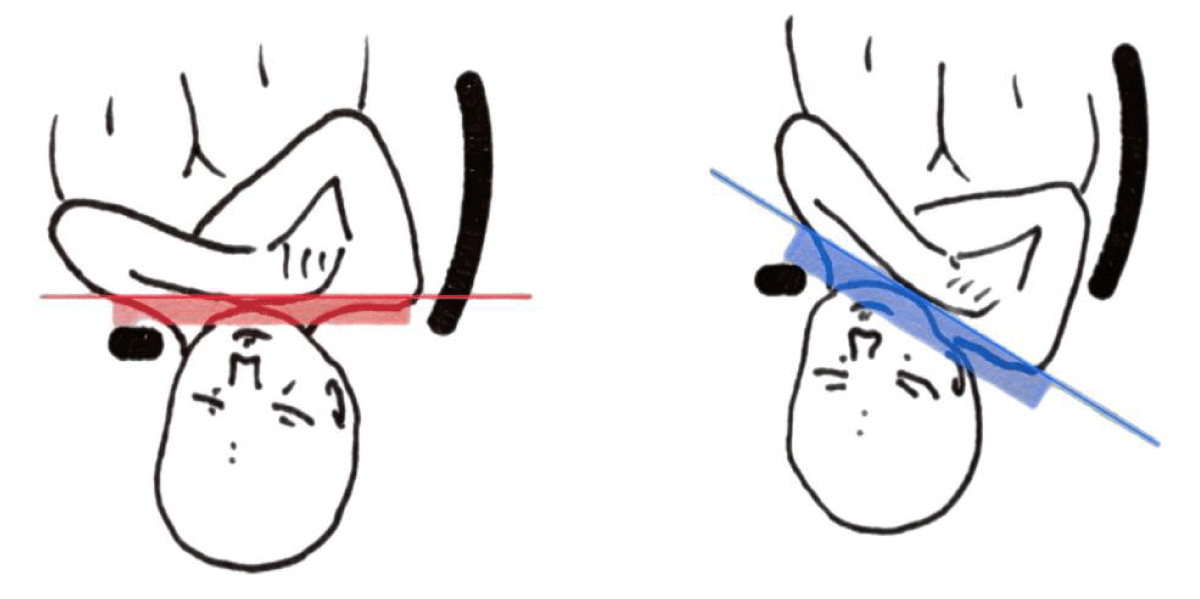
Figure 1: Creating the Tilt by pulling down the posterior shoulder.
The McRoberts Maneuver applied simultaneously with the efforts mentioned above to enter the infant in the pelvis, increased the diameter of the birth canal [26], allowing more space for the infant to proceed.
The presented method reaches the goal of the sling procedure [9] without causing possible injuries.
Comparing the main points of the above-described Tilt and Kristeller Procedure to other maneuvers could highlight their resemblance and difference.
Extracting and freeing the posterior shoulder—the Posterior Axilla Maneuver [4] —is a known maneuver to treat shoulder dystocia. It solves half of the task by delivering the posterior shoulder, offering a better grip for further manipulation, and preparing the posterior arm to be extracted, where possible. In severe cases, however, no additional manipulation is likely, e.g., trunk rotation or posterior arm delivery. Most current Posterior Axilla Maneuvers rely on rotation.
We could exaggerate the downward pull of the posterior shoulder during extraction so we could create the backward Tilt of the shoulder girdle and the anterior shoulder line and surface in the midsagittal plane, preparing it for a backward slide behind the symphysis. In contrast, the Holman Maneuver [6], which also is one of the first Posterior Axilla Maneuvers and forerunner of the procedure described above, pulls down the posterior shoulder only to a limited extent: 'as far as it will comfortably go' [6], therefore not comprising a pivotal point of it.
Most previous posterior axilla maneuvers do not explicitly focus on the exaggerated downward pull of the posterior shoulder [4], i.e., the Tilt of the shoulder girdle, as a precondition for further manipulation. However, in our procedure, it has an essential role. Pulling down the posterior shoulder while staying anterior in the original impacted position means the shoulder girdle is tilted backward in the median sagittal plane. Because the shoulders are connected, the anterior shoulder line and surface are tilted backward, too. It changes its relative position with which it contacts the back inner surface of the symphysis: from the original 90 degrees to a less impacting degree that further decreases with each downward move of the fetus. With these steps, the anterior impacted shoulder is freed. It's a prerequisite for any further exertion of forces. The Tilt also means the less functional diameter of the passing fetus against the bony birth canal.
One of the current methods that implicitly uses the Tilt advantage is the Sling procedure. This method, however, requires the rotation of the trunk, which could cause severe injuries and circular lacerations to the infant. In our method, there is no need to rotate the trunk—it was impossible—and although creating the Tilt, the infant escapes these injuries. In this sense, our method is a revised Sling procedure without implementing the sling itself.
After freeing the impacted anterior shoulder, we needed a driving force to move the fetus downward. We used the Kristeller procedure, which provided adequate force to move the stalled infant. The Kristeller procedure is the second important point in the procedure mentioned above that makes a difference. It has acted as a driving force to slide the fetus backward and downward, with the shoulder girdle, i.e., the anterior shoulder line, and surface now tilted backward in the midsagittal plane.
The Kristeller procedure is not usually allowed in shoulder dystocia. However, after freeing the impacted anterior shoulder, we could use it successfully.
In the Holman maneuver, fundal pressure is applied in the early phase of the Posterior Axilla Maneuver, and later, only the Rubin I. maneuver is carried out.
The first difference is the Kristeller procedure, which, in our method, is a core procedure carried out only after the posterior shoulder is extracted, e.g., the Tilt is created, not as a preliminary action as in the Holman procedure.
The second difference is the supra symphyseal push - in the direction of the maternal spine - to rotate the anterior shoulder within the pelvic inlet plane [6] - not in the direction of the axis of the birth canal - although to push the anterior axilla into the pelvis [6]. We have not focused on the rotation of the anterior shoulder nor the moving toward the back of the mother. The direction of the force of the Rubin I. maneuver is perpendicular to that of the Kristeller procedure, which facilitates the downward movement of the fetus.
The previously mentioned Sling procedure also exerts a great force, enough to make the fetus move. The Sling procedure requires the rotation of the trunk, too, but could come with the possible cost of severe injuries, namely circular lacerations. In our method, there is no need to rotate the trunk, and the infant escapes circular laceration injuries.
In shoulder dystocia, brachial plexus injuries are constantly questioned. Brachial plexus injury occurs when two points of the same-sided brachial plexus are grabbed, fixed, and pulled against each other. In our method, we do not hold the same-sided brachial plexus at two different points, nor do we pull against each other.
On the first possible questionable occasion, we grabbed the posterior shoulder, extracted and pulled it backward, now outside of the vagina, while the anterior shoulder was impacted. We grabbed the posterior shoulder while the opposite-sided, anterior shoulder was impacted and fixed. Usually and voluntarily in any person, it is possible to shrug both shoulders in the same direction or move the shoulders in the opposite direction.
On the second possible questionable occasion, we grabbed and pulled the extracted posterior shoulder to the back of the mother. At the same time, we pushed the anterior surface of the neck backward in the same direction. This move did not cause a brachial plexus injury.
On the third possible questionable occasion, the fetus was moved downward by the Kristeller procedure. Here, we did not have to exert any traction on the shoulders; we just kept the shoulders in their position till the infant was born. This move did not cause injuries either.
When grabbing the arm's posterior axilla and posterior upper part, we had to exert force to pull the posterior shoulder down. This move caused minor bruises and swelling to the upper part of the posterior arm. After birth, after a thorough pediatric examination, fractures and other injuries here and elsewhere were excluded.
Average birth process explanations rely on the movement of the head in the neck joints and trunk movements in the thoracal spine joints. Our method utilizes the complex movement of the shoulder shrug, including the clavicle, the thoracal spines, the upper arm, the scapula, and the corresponding joints. This method of delivery, however, is not unprecedented. Similar birth movements can also occur in preterm, low-birth-weight infants, where the classical term-birth movements do not apply.
Our method distantly resembles the Posterior Axilla Maneuvers described by Holman [6] and Menticoglou [8], respectively, and the Sling procedure described initially by Cluver and Hofmeyr [9-11]. However, when the anterior shoulder is inaccessible, and neither the posterior arm nor the trunk is movable, the known methods are not applicable.
The procedure mentioned above could be worth trying as a last resort before implementing more aggressive rescue maneuvers.
The advantages of our proposed method over existing Posterior Maneuvers can be summarized in a few points.
We delivered an infant weighing 5.140 gr (11 lbs. 5 oz.) from shoulder dystocia without long-term sequelae. Due to severe spatial constraints, the infant's movement has been limited in both direction and extent. We haven’t — because we couldn’t — moved the trunk in any other direction but downward to the outside of the perineum with the posterior hand grabbing the posterior shoulder and backward to the maternal sacrum with the anterior hand pushing the anterior side of the neck. This means that our method was applicable when no rotation was possible. Published case reports of successful deliveries from shoulder dystocia included infants who had less than this weight. We believe the proposed method can successfully address shoulder dystocia in the higher-than-current birth weight range.
Long-term complications frequently occur during deliveries with shoulder dystocia. Our method has avoided plexus injury — theoretically, most Posterior Axilla Maneuvers are exempt from plexus injury. In addition, our method did not involve rotation during the process, and no impact on the shoulders occurred in that direction. There has been no pull on the posterior shoulder but a Kristeller-type push on the fundus to move the infant along the birth canal. This also means that our process has avoided the possible injuries from the Sling procedure [27] and less traction and impact have been exerted on the posterior shoulder region.
The proposed maneuver has a broader range of applications regarding infant weight. Because of the tilt, it's still applicable with strict movement limitations when rotation is not feasible. It is safer than existing methods that require similar force generation to move the trunk — it’s a sling-type procedure without applying a sling but a Kristeller-type push.
Our proposed method could extend the operational range and enhance the safety characteristics.
Patient consent
The corresponding author declares that the patient agreed to publish her case on June 11, 2024.
Author's contributions
The authors state the following contributions:
Dr. László Sárközi
− Contributed substantially to the conception and design of the work.
− Drafted the work and critically reviewed it for important intellectual content.
− Approved the final version to be published.
− Agrees to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dr. András Hegedűs
- Contributed substantially to the conception of the work.
- Critically reviewed the work for important intellectual content.
- Approved the final version to be published.
- Agrees to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dr. István Péterfi
- Critically reviewed the work for important intellectual content.
- Approved the final version to be published.
- S2k guidelines for shoulder dystocia published. German Society for Gynecology and Obstetrics. Available from: https://www.dggg.de/presse/pressemitteilungen-und-nachrichten/s2k-leitlinie-zur-schulterdystokie-veroeffentlicht
- Habek D. Severe refractory bilateral shoulder dystocia released with digital hooking (Bourgeois-Siegemundin) manoeuvre. J Obstet Gynaecol. 2019;39(4):581. Available from: https://doi.org/10.1080/01443615.2018.1499077
- Dandurand M, Michel B, Fabre C, Stoebner P, Meunier L. Neonatal Volkmann's syndrome. Ann Dermatol Venereol. 2009;136(11):785-9. Available from: https://doi.org/10.1016/j.annder.2009.01.018
- Barbieri RL. Intractable shoulder dystocia: A posterior axilla maneuver may save the day. OBG Management. 2016;28(4):17-21. Available from: https://www.mdedge9-beta.mdedge.com/obgyn/article/107793/obstetrics/intractable-shoulder-dystocia-posterior-axilla-maneuver-may-save-day
- Phillips MH. Percival Willughby's observations in midwifery. J Obstet Gynaecol Br Emp. 1952;59(6):753-62. Available from: https://doi.org/10.1111/j.1471-0528.1952.tb14757.x
- Holman MS. A new manoeuvre for delivery of an impacted shoulder, based on a mechanical analysis. S Afr Med J. 1963;37:247-9. Available from: https://pubmed.ncbi.nlm.nih.gov/13961398/
- Schramm M. Impacted shoulders--a personal experience. Aust N Z J Obstet Gynaecol. 1983;23(1):28-31. Available from: https://doi.org/10.1111/j.1479-828x.1983.tb00154.x
- Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108(3 Pt 2):755-7. Available from: https://doi.org/10.1097/01.aog.0000232505.65290.04
- Cluver CA, Hofmeyr GJ. Posterior axilla sling traction: a technique for intractable shoulder dystocia. Obstet Gynecol. 2009;113(2 Pt 2):486-488. Available from: https://doi.org/10.1097/aog.0b013e318190a2d6
- Hofmeyr GJ, Cluver CA. Posterior axilla sling traction for intractable shoulder dystocia. BJOG. 2009;116(13):1818-20. Available from: https://doi.org/10.1111/j.1471-0528.2009.02373.x
- Cluver CA, Hofmeyr GJ. Posterior axilla sling traction for shoulder dystocia: case review and a new method of shoulder rotation with the sling. Am J Obstet Gynecol. 2015;212(6):784.e1-7. Available from: https://doi.org/10.1016/j.ajog.2015.02.025
- Hoek J, Verkouteren B, van Hamont D. Posterior axilla sling traction: a new technique for severe shoulder dystocia. BMJ Case Rep. 2019;12(3):e226882. Available from: https://doi.org/10.1136/bcr-2018-226882
- Taddei E, Marti C, Capoccia-Brugger R, Brunisholz Y. Posterior axilla sling traction and rotation: A case report of an alternative for intractable shoulder dystocia. J Obstet Gynaecol. 2017;37(3):387-389. Available from: https://doi.org/10.1080/01443615.2016.1264070
- Sancetta R, Khanzada H, Leante R. Shoulder Shrug Maneuver to Facilitate Delivery During Shoulder Dystocia. Obstet Gynecol. 2019;133(6):1178-1181. Available from: https://doi.org/10.1097/aog.0000000000003278
- Ansell L, Ansell DA, McAra-Couper J, Larmer PJ, Garrett NKG. Axillary traction: An effective method of resolving shoulder dystocia. Aust N Z J Obstet Gynaecol. 2019;59(5):627-633. Available from: https://doi.org/10.1111/ajo.13029
- Lau SL, Sin WTA, Wong L, Lee NMW, Hui SYA, Leung TY. A critical evaluation of the external and internal maneuvers for resolution of shoulder dystocia. Am J Obstet Gynecol. 2024;230(3S):S1027-S1043. Available from: https://doi.org/10.1016/j.ajog.2023.01.016
- Tan TS, Mohamed A, Dharmaraj S. Bilateral fractures in a shoulder dystocia delivery. BMJ Case Rep. 2016;2016:bcr2016217762. Available from: https://doi.org/10.1136/bcr-2016-217762
- Thompson KA, Satin AJ, Gherman RB. Spiral fracture of the radius: an unusual case of shoulder dystocia-associated morbidity. Obstet Gynecol. 2003;102(1):36-8. Available from: https://doi.org/10.1016/s0029-7844(03)00487-3
- Mottet N, Bonneaud M, Eckman-Lacroix A, Ramanah R, Riethmuller D. Active delivery of the anterior arm and incidence of second-degree perineal tears: a clinical practice evaluation. BMC Pregnancy Childbirth. 2017 12;17(1):141. Available from: https://doi.org/10.1186/s12884-017-1322-8
- Ruis KA, Allen RH, Gurewitsch ED. Severe shoulder dystocia with a small-for-gestational-age infant: a case report. J Reprod Med. 2011;56(3-4):178-80. Available from: https://pubmed.ncbi.nlm.nih.gov/21542540/
- Sentilhes L, Sénat MV, Boulogne AI, Deneux-Tharaux C, Fuchs F, Legendre G, et al. Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol. 2016;203:156-61. Available from: https://doi.org/10.1016/j.ejogrb.2016.05.047
- O'Shaughnessy MJ. Hysterotomy facilitation of the vaginal delivery of the posterior arm in a case of severe shoulder dystocia. Obstet Gynecol. 1998;92(4 Pt 2):693-5. Available from: https://doi.org/10.1016/s0029-7844(98)00153-7
- Ansell Irving L, McAra-Couper J, Smythe E. Shoulder dystocia: a qualitative exploration of what works. Midwifery. 2012;28(4):E461-8. Available from: https://doi.org/10.1016/j.midw.2011.05.007
- Robson M. Shoulder dystocia: Is it time to think differently? Aust N Z J Obstet Gynaecol. 2019;59(5):605-607. Available from: https://doi.org/10.1111/ajo.13060
- Whittington JR, Poole AT. Introduction of Posterior Axilla Sling Traction in Simulated Shoulder Dystocia. AJP Rep. 2018;8(4):e247-e250. Available from: https://doi.org/10.1055/s-0038-1675350
- Martius G. Obstetric-perinatological operations. 1986;143.
- McCarter AR, Theiler RN, Rivera-Chiauzzi EY. Circumferential shoulder laceration after posterior axilla sling traction: a case report of severe shoulder dystocia. BMC Pregnancy Childbirth. 2021;21(1):45. Available from: https://doi.org/10.1186/s12884-020-03526-2