
More Information
Submitted: May 14, 2024 | Approved: May 24, 2024 | Published: May 27, 2024
How to cite this article: Siati A, Ghaddou Y, Sair K, Dehayni M. Successful Management of a Giant Splenic Cyst during Pregnancy: A Rare Case. Clin J Obstet Gynecol. 2024; 7: 069-071.
DOI: 10.29328/journal.cjog.1001167
Copyright License: © 2024 Siati A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Splenic cyst; Pregnancy; Surgical management

Successful Management of a Giant Splenic Cyst during Pregnancy: A Rare Case
Abderrahim Siati1* , Youssef Ghaddou, Khalid Sair2 and Mohamed Dehayni2
, Youssef Ghaddou, Khalid Sair2 and Mohamed Dehayni2
1Department of Gynecology and Obstetrics, Sheikh Khalifa Ibn Zaid International University Hospital, Mohammed VI University of Sciences and Health, Casablanca, Morocco
2Department of Visceral and Digestive Surgery, Sheikh Khalifa Ibn Zaid International University Hospital, Mohammed VI University of Sciences and Health, Casablanca, Morocco
*Address for Correspondence: Abderrahim Siati, Department of Gynecology and Obstetrics, Sheikh Khalifa Ibn Zaid International University Hospital, Mohammed VI University of Sciences and Health, Casablanca, Morocco, Email: [email protected]
Background: Maternal splenic cyst during pregnancy appears to be a rare pathology whose treatment is not codified. The most feared complication is rupture during pregnancy. It occurs in 60% of cases in the third trimester of pregnancy, leading to significant maternal-fetal morbidity and mortality.
Case report: We describe the successful management of a 24-year-old patient, G1P0, with a history of a recurrent splenic cyst. She presented with a giant splenic cyst measuring 28 cm in diameter at 30 weeks of amenorrhea. A cesarean section was performed at 37 weeks gestation. A splenectomy was performed on day 21 postpartum.
Conclusion: The incidence of splenic cysts is extremely rare during pregnancy. The diagnosis must be made as early as possible to undertake appropriate treatment before the appearance of maternal-fetal complications.
The diagnosis of a splenic cyst during pregnancy is very rare, with a minimal number of cases reported in the literature. Splenic cysts are often discovered incidentally because they are rarely symptomatic. The most frightening complication is rupture during pregnancy, especially during the third trimester. To our knowledge, there is no defined protocol for managing this pathology, which differs depending on the teams and the term of the pregnancy. We describe the successful management of a giant splenic cyst during pregnancy. A splenectomy was decided taking into account the recurrent context of this cyst.
24-year-old patient, primigravida, with a history of laparoscopic removal of a splenic cyst two years ago. She presented to our structure for a pain syndrome at 30 weeks of gestation. Clinical examination revealed a large mass in the left hypochondrium (Figure 1). Ultrasound and Magnetic Resonance Imaging (MRI) revealed a large splenic cyst, located in the abdominopelvic region, with a thin wall and homogeneous fluid content, measuring 28 x 20 x 17 cm (Figure 2). Outpatient follow-up was carried out up to 37 weeks. Following the sudden onset of abdominal pain, the patient was hospitalized. The obstetric examination showed the beginning of uterine contractions with the cervix open to 2 cm. An emergency cesarean section was indicated for acute fetal distress, allowing extraction of a male neonate weighing 3,200 g. A Pfannenstiel incision was made and for safety reasons: the fetal extraction was carried out by instrumental means, the uterus was not exteriorized and any maneuver likely to cause rupture of the cyst was avoided. The postoperative course was simple. A control abdominal and pelvic CT scan was performed 7 days after delivery. Subsequently, the patient was entrusted to the visceral surgery team. Given the recurrent nature of the cyst, a splenectomy was performed 21 days postpartum via a midline supraumbilical laparotomy (Figure 3). Pathological examination revealed a simple epithelial cyst without signs of malignancy.
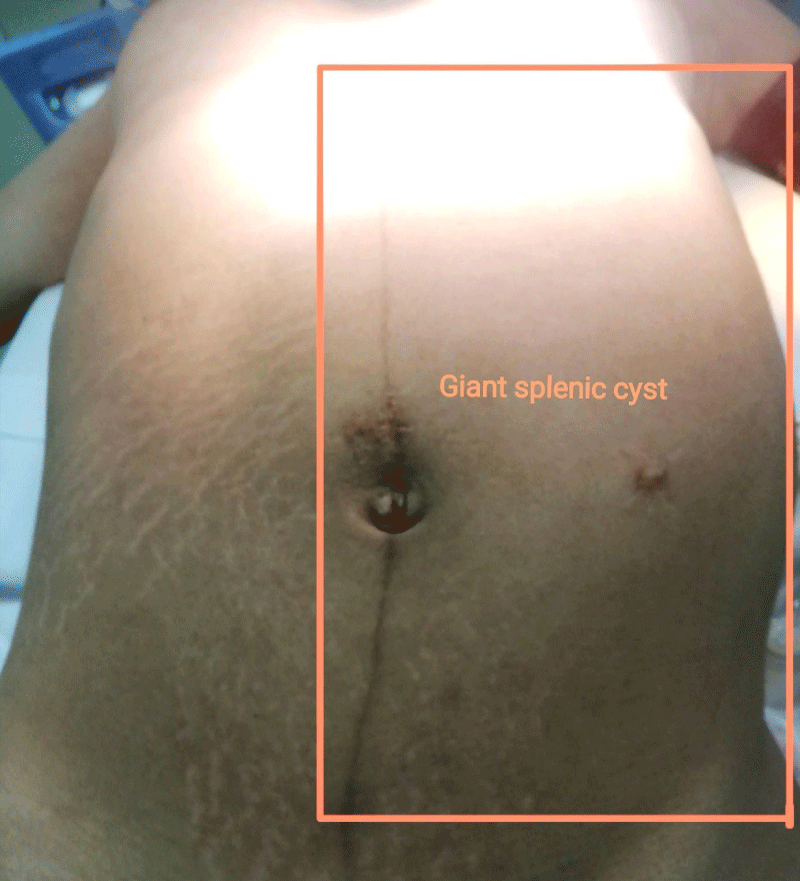
Figure 1: Clinical examination revealed a large mass in the left hypochondrium.
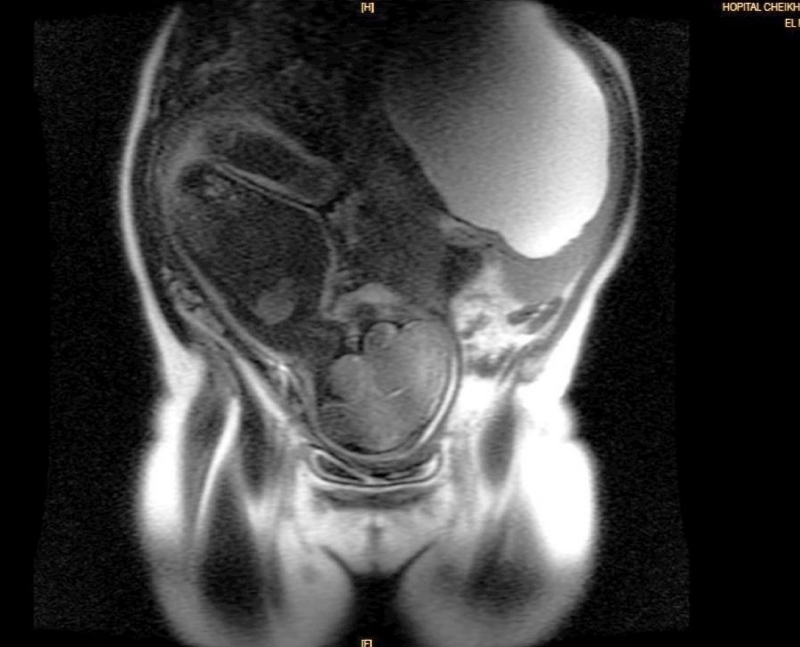
Figure 2: Magnetic Resonance Imaging (MRI) showing a large splenic cyst with the fetus, located in the abdominopelvic region.
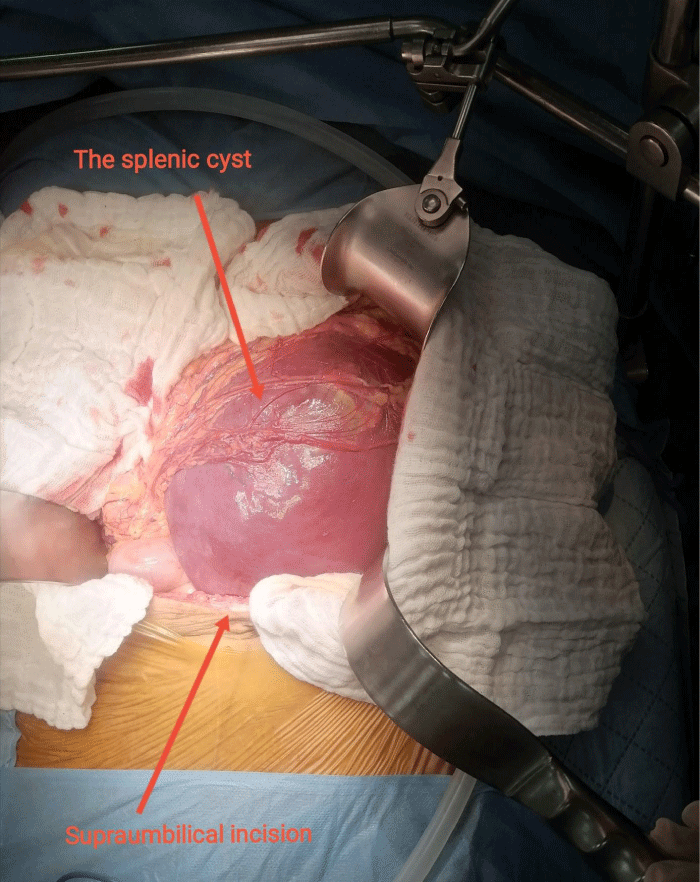
Figure 3: The macroscopic appearance of the splenic cyst.
The incidence of splenic cysts in the general population is very low, with approximately 800 cases published in the literature, and extremely rare during pregnancy (less than ten cases described) [1]. Splenic cysts can be of two types, primary or secondary, with etiologies: congenital, parasitic, neoplastic, or traumatic.
The most contributory exploration examination remainsMRI which surpasses ultrasound for its diagnostic performance and characterization of the lesion and falls within the framework of a preoperative assessment [1].
The complications are hemorrhagic or infectious, which can be complicated depending on the nature of the cyst by hemoperitoneum, peritonitis, or anaphylactic shock in the case of a hydatid cyst [1,2]. In the event of rupture, this occurs in 60% of cases in the third trimester of pregnancy. The maternal-fetal mortality rate in the event of hemorrhagic rupture of the cyst during labor is up to 70% [1]. The diagnosis of splenic cyst must therefore be made as early as possible during pregnancy to undertake appropriate treatment before the appearance of maternal-fetal complications.
In the literature, surgical or radiological treatment is recommended in the second trimester if the cyst is symptomatic or measures more than 5 cm in the long axis to avoid the risk of complications at the end of pregnancy [1]. Surgical treatment must be the least invasive to preserve the hematopoietic and immune systems. The choice of therapy, radiological or surgical, depends on the size of the cyst, the term of the pregnancy, the patient's condition, and the technical possibilities. Splenectomy should only be performed in the presence of a suspicious-looking cyst or in the event of splenic rupture [3]. Planned surgical management is recommended, whenever possible by laparoscopic way. The treatments described consist of fenestration of the cyst with secondary omentopexy on the residual part. Conservative treatment by transcutaneous puncture alone was described for the first time in 2006 with recurrence of the cyst during pregnancy [4].
In our case, the decision for splenectomy was taken taking into account the recurrent nature of the cyst. The surgery was scheduled for day 21 postpartum and the patient expressed her consent. Outside of pregnancy, percutaneous drainage with or without alcohol is an effective alternative to surgery [5]. Monthly clinical and ultrasound monitoring is possible for asymptomatic cysts less than 5 cm due to possible spontaneous disappearance [6]. The success rate of a puncture-drainage is around 80% according to studies [7]. Combined with alcohol, puncture drainage helps limit the risk of rupture of the cyst during work by reducing its volume.
Regarding the delivery way, it depends on obstetric conditions. The indication for systematic cesarean section does not seem legitimate. Delivery must be planned, possibly considering assistance with expulsion, to limit the risk of rupture secondary to intraabdominal hyperpressure.
To avoid complications, early treatment in the second trimester is desirable if the cyst is symptomatic or measures more than 5 cm in the long axis. For smaller cysts: simple regular ultrasound monitoring is preferable. Management should preferably be radiological to avoid anesthetic and surgical complications before the third trimester. Splenectomy is reserved for a suspicious or recurrent cyst or in the case of splenic rupture.
Consent
The patient's consent has been received for publishing the personal information for research and studies
Author’s Contribution
All the authors have read and agreed to the final manuscript.
- Rotas M, Ossowski R, Lutchman G, Levgur M. Pregnancy complicated with a giant splenic cyst: a case report and review of the literature. Arch Gynecol Obstet. 2007 Apr;275(4):301-5. doi: 10.1007/s00404-006-0229-9. Epub 2006 Aug 26. PMID: 16937120.
- Balzan SM, Riedner CE, Santos LM, Pazzinatto MC, Fontes PR. Posttraumatic splenic cysts and partial splenectomy: report of a case. Surg Today. 2001;31(3):262-5. doi: 10.1007/s005950170183. PMID: 11318135.
- Buchsbaum HJ. Splenic rupture in pregnancy. Report of a case and review of the literature. Obstet Gynecol Surv. 1967 Jun;22(3):381-95. PMID: 4859770.
- Montasser AM, Roger B, Marwan F, Felicity A. Conservative management of gigantic splenic cyst during pregnancy; a differential diagnosis for chest pain caused by the forgotten organ. Gynecol Surg. 2010; 7:49-51.
- Singh AK, Shankar S, Gervais DA, Hahn PF, Mueller PR. Image-guided percutaneous splenic interventions. Radiographics. 2012 Mar-Apr;32(2):523-34. doi: 10.1148/rg.322115135. PMID: 22411947.
- Wolters U, Keller HW, Lorenz R, Pichlmaier H. Milzzysten: Indikation zur Operation und operatives Vorgehen [Splenic cysts: indications for surgery and surgical procedures]. Langenbecks Arch Chir. 1990;375(4):231-4. German. doi: 10.1007/BF00187444. PMID: 2203951.
- Kang M, Kalra N, Gulati M, Lal A, Kochhar R, Rajwanshi A. Image guided percutaneous splenic interventions. Eur J Radiol. 2007 Oct;64(1):140-6. doi: 10.1016/j.ejrad.2007.02.011. Epub 2007 Mar 19. PMID: 17374470.