Case Report
A Rare case of synchronous primary malignancies of gall bladder and ovary

Ridhi Narang*, T Das, M Dagar, M Srivastava, S Bhalla and I Ganguli
Institute of obstetrics and gynecology, Sir Gangaram Hospital, New Delhi, India
*Address for Correspondence: Ridhi Narang, Institute of Obstetrics and Gynecology, Sir Gangaram Hospital, New Delhi, India, Tel: +91 0 8947933115; Email: [email protected]
Dates: Submitted: 03 August 2018; Approved: 05 September 2018; Published: 06 September 2018
How to cite this article: ONarang R, Das T, Dagar M, Srivastava M, Bhalla S, et al. A Rare case of synchronous primary malignancies of gall bladder and ovary. Clin J Obstet Gynecol. 2018; 1: 052-055. DOI: 10.29328/journal.cjog.1001008
Copyright License: © 2018 Narang R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Introduction
A malignant tumor has the capacity to grow rapidly and to metastasize to the other parts of the body. Ovary has been a common organ for secondaries caused by hematological spread of the tumor and exhibits the same histopathology as that of the primary tumor.
Very rarely, it has been found that the patients suffer from two or more histologically distinct, simultaneously detected malignancies, which are called as synchronous tumors or multiple primaries [1]. These multiple primaries can have an impact on cancer treatment (e.g., surgery) and affect the overall prognosis of the patient. Although there is no consensus on the definition of synchronous cancer, commonly two or more primary tumors that occur in a patient closely with respect to the time interval are termed as synchronous tumors [2].
Simultaneous diagnosis of gall bladder carcinoma with ovarian carcinoma with distinct histopathology is rare. A very few cases have been reported so far in literature. We discuss here a rare case that presented with synchronous tumor of gall bladder and the ovary.
Case Report
A 48 years old female, presented with complains of post-menopausal bleeding and pain abdomen since one and half months, associated with feeling of distension of abdomen. The abdominal distension was present with mild tenderness in umbilical and epigastric regions. The patient attained menopause 2 years back, her previous menstrual cycles were regular and she had an episode of postmenopausal bleeding around ten days before presentation. She has been married for last 29 years and she was P2L2, both normal vaginal deliveries. She was a known case of hypertension and hypothyroidism and was on the medication for the same.
The patient had a strong family history of carcinoma. Her sister and mother had ovarian cancer. Her grandmother also died of some cancer, which the patient could not recall.
On examination, her vitals were stable. On per abdomen examination, nontender, irregular size (10x8cm) abdominopelvic mass felt which was cystic in consistency. On per vaginum examination, uterus was retroverted; 8weeks size with restricted mobility, through right fornix the mass was felt, with left fornix free.
Endometrial cells were seen on LBC. Ultrasonography revealed a polypoidal Gall bladder mass and a Cystic pelvic mass of 14.5x 12 x9.5 cm, with irregular peripheral solid component with intra cystic excrescences and fine low level internal echos, extending from the right adnexa to the left side with no internal vascularity. Mild free fluid was seen in pelvis.
MRI was suggestive of diffuse thickening of endometrium 15.9mm along the anterior wall s/o diffuse adenomyosis. Well-defined solid cystic mass in pelvis and lower abdomen with solid component showing restricted diffusion; possibility of Krukenberg’s tumor and minimal ascites was seen. A well-defined lobulated soft tissue mass arising from anterior and right lateral wall of gall bladder, projecting into the body of gall bladder lumen with restricted diffusion s/o neoplastic etiology.
Surprisingly, all tumor markers were in normal range i.e. CEA: 1.86, HE4: 229.9, CA125: 32, LDH: 161, AFP: 2.1, BetaHCG: 1.5 and C19-9: 2.0 Other routine investigations were done including mammography which was suggestive of small fibro adenoma of right breast, left breast – cyst and bilateral prominent axillary lymph node: likely to be reactive.
Patient was taken up for laparotomy, proceeded to radical hysterectomy, bilateral pelvic lymphadenectomy, appendicectomy, total omentectomy with radical cholecystectomy under general and epidural anesthesia. On right side 15x10 cm solid to cystic ovarian tumor noted. Uterus around 8 weeks size, right tube stretched over the tumor, left tube and ovary adhered to tumor. Peritoneal washings were taken. Frozen section of the right ovarian tumor was reported as borderline serous tumor, left ovary was reported as adenocarcinoma of the ovary and the gallbladder as moderately differentiated adenocarcinoma. The postoperative period was uneventful.
The final histopathology report was suggestive of serous carcinoma of both ovaries and right fallopian tube (Figure 1), moderately differentiated adenocarcinoma of Gall bladder (Figure 2). Lymph nodes were free of tumor. The endometrium was in proliferative phase, myometrium had adenomyosis with cervix showing features of chronic cervicitis and both side parametria was free of tumor.
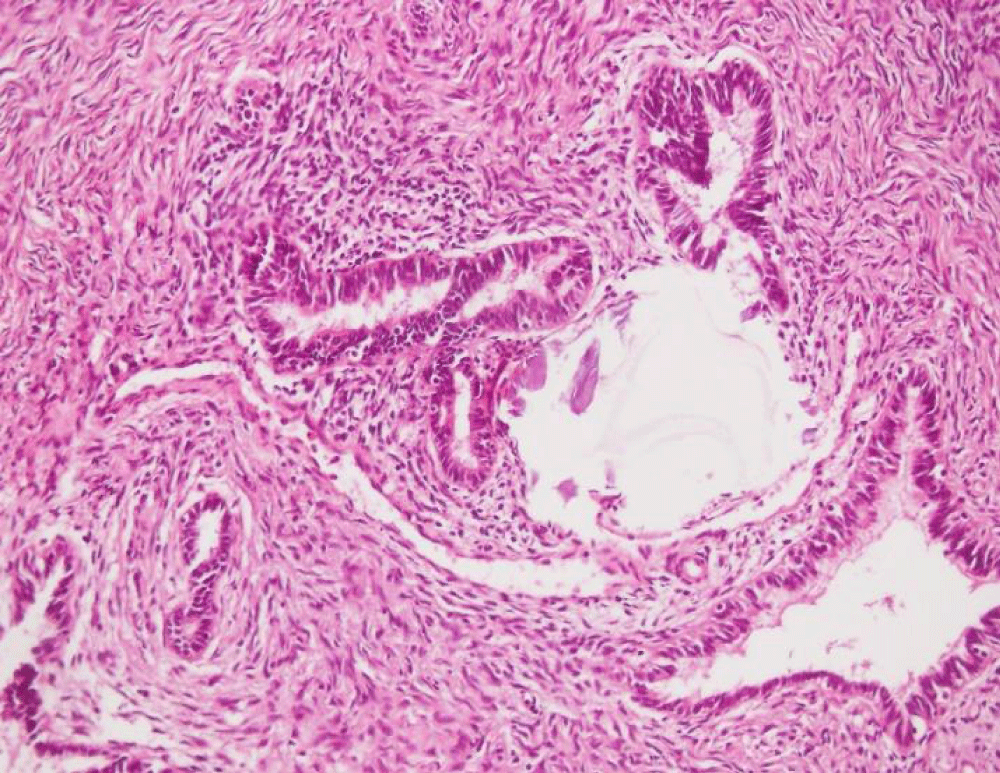
Figure 1: Section from the ovarian tumor shows cystic tumor lined by complex branching papillae, the papillae wall lined by multiple layers of tumor cells showing hyper chromatic nuclei, nuclear pleomorphism and moderate eosinophilic cytoplasm.
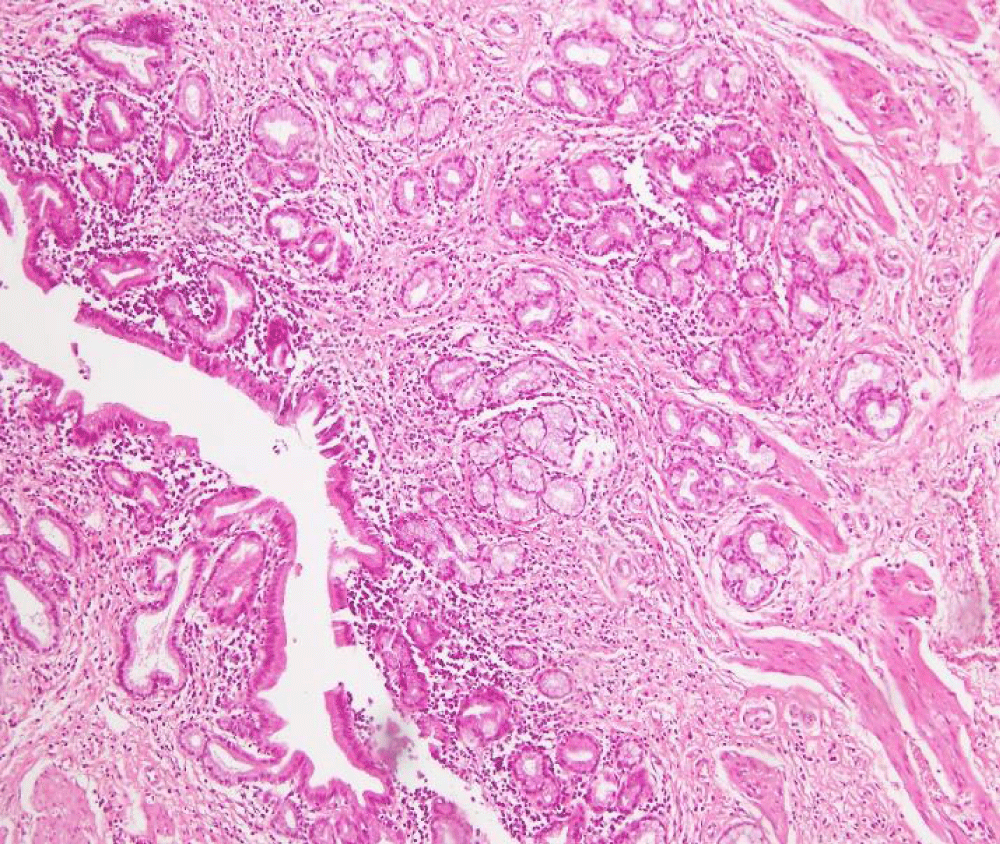
Figure 2: Section from gallbladder showed exophytic tumor composed of closely packed papillae and solid pattern with tumor cells showing brisk mitotic activity.
Ovarian tumor was positive for CA 125, WT1, ER, PR and PAX8. P53 was positive in almost 100% cases but CA19.9 was negative. GALL BLADDER TUMOR was focally positive for CA19.9, CA125 and WT1 but was negative for ER, PR and PAX8. P53 was positive in few cells.
Patient received six cycles of chemotherapy with nanoxel and carboplatin post operatively. She is doing well and is healthy after one year of treatment.
Discussion
It is very rare to find multiple primary malignancies with different histopathology occurring simultaneously and very few cases of multiple primaries have been reported in literature so far.
Jarvi et al. [3], reported a case of gall bladder adenocarcinoma with bilateral benign serous cyst adenoma of ovaries with deposits of metastatic adenocarcinoma. The conclusion of their study was that careful evaluation of the digestive tract should be considered in a patient presenting with ovarian masses. In their case, earlier they thought of cancer gall bladder with metastasis to ovary, which presented as ovarian torsion. But histology revealed them to be two distinct primary cancers as it was seen in our case.
Majority of reported cases have been either gall bladder carcinoma with ovarian metastasis or ovarian carcinoma with metastasis to gall bladder 4-6.
Bassi et al. [4], presented a rare combination of an ovarian carcinoid synchronous with gallbladder carcinoid. They concluded that a very rare case of a synchronous combination of ovarian with gall bladder carcinoid has been successfully managed with a multidisciplinary approach; however, long-term follow-up is needed.
Ozan et al. [5], reported a case with three synchronous tumors in a 52-year-old patient including a uterine endometrioid adenocarcinoma, a mucinous adenocarcinoma of the gallbladder, and an ovarian endometrioid carcinoma with a clear cell component. They did a total abdominal hysterectomy with bilateral salpingo-oophorectomy, bilateral pelvic and Para aortic lymph node dissection, partial omentectomy and cholecystectomy. They did cholecystectomy for a perioperative incidental suspicious nodule on the serosal surface of the gallbladder but in our case the diagnosis of gall bladder pathology was done preoperatively, but the two distinct histopathology report proved that they were synchronous primary tumors.
Our patient presented with two primaries, gall bladder malignancy together with ovarian malignancy. This case could have been passed off as Krukenberg tumor of the ovary arising from gall bladder as primary. But careful histopathological and immunochemical examination proved that these two were distinct primary tumors. The correct histopathological diagnosis is very important for deciding the line of management of these patients. We could manage her efficiently because of the careful diagnosis. Our patient is absolutely fine after the complete chemotherapy.
Conclusion
To conclude synchronous primary tumors is a rare condition. A careful clinical work up, complete surgical management, accurate histopathological diagnosis goes a long way in managing these rare conditions. Our patient had good outcome because of accurate clinical suspicion and appropriate management.
Contribution of the Authors
Dr. Indrani Ganguli, chairperson, Head of the department, institute of obstetrics and gynecology, Sir Gangaram Hospital, New Delhi, encouraged to do the scientific work.
Dr. S. Bhalla, senior consultant in pathology department contributed by helping in understanding the histopathological findings.
Dr. Mala Srivastava, professor GRIPMER and senior consultant, institute of obstetrics and gynecology, Sir Gangaram Hospital helped in surgical management of the patient.
Dr. Mamta Dagar, senior consultant, institute of obstetrics and gynecology, Sir Gangaram Hospital organized the patient care.
Dr. Tarun K. Das, associate consultant, institute of obstetrics and gynecology, Sir Gangaram Hospital helped in writing the manuscript.
Dr. Ridhi Narang, senior resident, institute of obstetrics and gynecology, Sir Gangaram Hospital, is the corresponding author of the manuscript.
There is no conflict of interests that I should disclose and I have no relevant financial interests/funding in this manuscript. Informed consent was taken from the patient and relatives before submitting the manuscript and the ethical standards were followed.
References
- Synchronous Cancer. Segen's Medical Dictionary. (2011). Ref.: https://goo.gl/7Aucmj
- Woodruff JD, Solomon D, Sullivant H. Multifocal disease in the upper genital canal. Obstet Gynecol 1985; 65: 695–698. Ref.: https://goo.gl/PHpoKu
- Ozan H, Ozerkan K, Aker S, Bülbül M. A case with three primary tumors of the ovary, endometrium and gallbladder. Eur J Gynaecol Oncol 2008; 29: 551-553. Ref.: https://goo.gl/yr3QNU
- Bassi R, Arora R, Bhasin S, Khurana N. An Unusual Case of Synchronous Carcinoid of Ovary and Gall Bladder. Case Reports in Obstetrics and Gynecology. 2013; 2013: Article ID 737016. 3. Ref.: https://goo.gl/C7xrkA
- Jarvi K, Kelty CJ, Thomas WE, Gillespie A. Bilateral ovarian metastases from carcinoma of the gallbladder. Gynecol Oncol 2006; 103 :361–362. Ref.: https://goo.gl/FHwx2Y